
부갑상선 호르몬 상승 상태에서 처음 관찰한 부갑상선 지방선종, 주변 갑상선과 구별해서 유무의 판단이 필요 - 동대문구 답십리, 전농동, 우리안애 우리안愛 내과
- 4월 21일
- 5분 분량
70대 초반 남자, 21년부터 진료 및 투약 - 혈압/고지혈
24년에 본원에서 첫 정기 평가, 혈압등 만성질환 환자에 포함된 칼슘수치가 10.5
10 이상이 나오는 경우가 적지 않고, PTH가 대부분 정상이라 보통은 큰 의심을 하지 않는데... 따라서, 다음 검사시 pth와 같이 추적을 계획

25년 추적시 ca은 오히려 경계값은데, 확인흔 PTH는 증가되어 있다.

설명후 갑상선/부갑상선 초음파 및 추적을 상의함
2개월뒤 시행
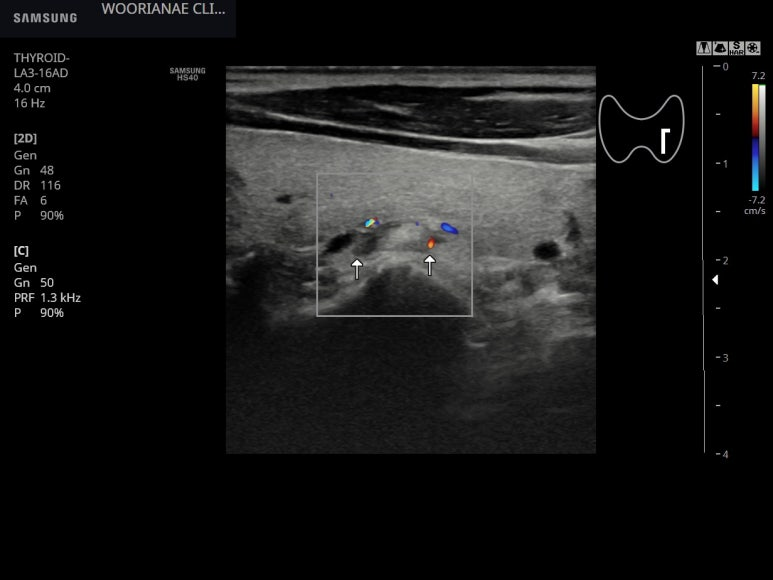
놓치기 쉬운 모양인데 갑상선 실질과 비슷한 음영의 결절이 갑상선의 후면에 위치하고
주변에 저음영이 있어 경계는 구별되나 전체적으로 고음영은 일반적인 부갑상선의 모습은 아닐수 있다.



추적한 PTH는 비슷하게 올라가 있는 모습, 재확인됨

진료 보면서 처음 맞닥트린 초음파 소견으로서... 서칭을 몇번에 걸쳐 해보다가 일치하는 상황 및 용어를 확인할수 있었다.
; 같은 모습, parathyroid lipoadenoma

Parathyroid lipoadenoma is an unusual variant of primary hyperparathyroidism (PHPT). It consists of hyperfunctioning parathyroid cell nests in abundant fatty stroma. Otherwise fat-containing lesions of endocrine glands are uncommon. It resembles lipoma rather than adenoma. Chow et al.[1] defined it as single parathyroid adenoma with more than 50% fat on histologic examination in conjunction with PHPT and resolution of hypercalcemia postoperatively. The World Health Organization defines parathyroid lipoadenoma as a “hamartoma-like benign neoplasm containing both chief cells and prominent stromal elements.”[2] Nonfunctional parathyroid lipoadenomas have also been reported.[3] Normally, fat occupies approximately 25% of adult parathyroid gland, and it increases with age and obesity.[4]
부갑상선 지방선종은 원발성 부갑상선기능항진증(PHPT)의 드문 변형입니다. 이는 풍부한 지방 기질 내에 과기능성 부갑상선 세포 덩어리로 구성됩니다. 내분비선에 지방을 함유하는 병변은 흔하지 않습니다. 이는 선종보다는 지방종과 유사합니다. Chow 등[1]은 PHPT와 수술 후 고칼슘혈증이 해소된 상태에서 조직학적 검사상 50% 이상의 지방을 함유하는 단일 부갑상선 선종으로 정의했습니다. 세계보건기구(WHO)는 부갑상선 지방선종을 "주세포와 현저한 기질 요소를 모두 함유하는 과오종과 유사한 양성 신생물"[2]로 정의합니다. 비기능성 부갑상선 지방선종도 보고된 바 있습니다.[3] 일반적으로 성인 부갑상선은 지방이 약 25%를 차지하며, 나이와 비만에 따라 증가합니다.[4]
In 1958, Ober and Kaiser[5] described parathyroid lipoadenoma for the first time in an asymptomatic 43-year-old male and termed it as “hamartoma of the parathyroid.” It has also been reported as parathyroid lipohyperplasia[6] and parathyroid adenoma with myxoid stroma.[7] The term “parathyroid lipoadenoma” was coined in 1962 by Abul-Haj et al.[8] Parathyroid lipoadenomas can occur at any age group but are more common among middle-aged females.[6,9] Clinical features and laboratory investigations of parathyroid lipoadenoma resemble that of usual parathyroid adenoma. Approximately 60 cases of parathyroid lipoadenoma have been reported so far. The rarity of the entity and resemblance with normal parathyroid tissue microscopically makes its diagnosis difficult.
1958년 Ober와 Kaiser[5]는 무증상 43세 남성에서 부갑상선 지방선종을 처음으로 기술하고 이를 "부갑상선 과오종"이라고 명명했습니다. 이 질환은 부갑상선 지방증[6] 및 점액성 기질을 가진 부갑상선 선종[7]으로도 보고되었습니다. "부갑상선 지방선종"이라는 용어는 1962년 Abul-Haj 등이 만들었습니다.[8] 부갑상선 지방선종은 모든 연령대에서 발생할 수 있지만 중년 여성에게 더 흔합니다.[6,9] 부갑상선 지방선종의 임상 양상 및 실험실 검사 결과는 일반적인 부갑상선 선종과 유사합니다. 현재까지 약 60건의 부갑상선 지방선종 사례가 보고되었습니다. 이 질환의 희귀성과 현미경적 소견이 정상 부갑상선 조직과 유사하기 때문에 진단이 어렵습니다.
In previously reported cases, approximately 64% cases had symptomatic disease, 28% were asymptomatic, and 7% had questionable symptoms.[13] Unlike parathyroid adenomas, they are not associated with multiple endocrine neoplasias or familial hyperparathyroidism. Parathyroid lipoadenoma is difficult to detect on preoperative imaging, may be due to high-fat content. Nuclear scan in our patient was not able to detect any lesion. The comparative differences between parathyroid lipoadenoma and classic parathyroid adenoma are mentioned in Table 1.
이전에 보고된 사례에서는 약 64%가 증상을 보였고, 28%는 무증상이었으며, 7%는 증상이 불확실했습니다.[13] 부갑상선 선종과는 달리, 부갑상선 지방선종은 다발성 내분비 종양이나 가족성 부갑상선기능항진증과 관련이 없습니다. 부갑상선 지방선종은 지방 함량이 높아 수술 전 영상 검사에서 발견하기 어려울 수 있습니다. 본 환자의 핵의학 검사에서는 병변이 발견되지 않았습니다. 부갑상선 지방선종과 전형적인 부갑상선 선종의 비교 차이점은 표 1에 제시되어 있습니다.

We conclude that due to rarity of the entity, parathyroid lipoadenoma as a cause of PHPT may be overlooked. Hence, knowledge of this entity is necessary to ensure that it does not get unnoticed as a cause of PHPT.
본 연구 결과는 부갑상선 지방선종이 매우 드문 질환이기 때문에 원발성 부갑상선기능항진증(PHPT)의 원인으로 간과될 수 있음을 시사합니다. 따라서 부갑상선 지방선종이 PHPT의 원인으로 간과되지 않도록 이에 대한 지식을 갖추는 것이 중요합니다.
상급병원 내분비내과 진료보기를 상의하였으나 우선 추적을 원하여 ... 6개월뒤 추적하기로 함
남자 골밀도 급여기준 나이를 이제 넘어서 골밀도 검사에 대한 상의도 함
here is considerable variation in who is considered for surgical treatment of primary hyperparathyroidism (PHPT). Indications for surgery for symptomatic disease include the presence of end organ damage such as renal stones or reduced bone mineral density. There is much debate over whether surgery should be considered for people who are asymptomatic. In the UK, most practice adheres to the National Institute for Health consensus guidelines. They recommend surgery for the following indications:
Serum calcium (>upper limit of normal): 1.0 mg/dL (0.25 mmol/L);
BMD by DXA: T-score ≤2.5 at lumbar spine, total hip, femoral neck, or distal 1/3 radius;
Vertebral fracture by x-ray, CT, MRI, or VFA;
Creatinine clearance <60 cc/min; 24-h urine for calcium >400 mg/d (>10 mmol/d) and increased stone risk by biochemical stone risk analysis;
Presence of nephrolithiasis or nephrocalcinosis by x-ray, ultrasound, or CT;
<50 years
It is relevant to consider the evidence base underpinning these consensus-based US recommendations.
원발성 부갑상선기능항진증(PHPT)의 수술적 치료 대상에는 상당한 차이가 있습니다. 증상이 있는 질환에 대한 수술 적응증에는 신장 결석이나 골밀도 감소와 같은 장기 손상이 포함됩니다. 무증상 환자에게 수술을 고려해야 하는지에 대해서는 많은 논쟁이 있습니다. 영국에서는 대부분의 의료기관이 국립보건원(NIH)의 합의 지침을 따릅니다. 이 지침에서는 다음과 같은 적응증에 대해 수술을 권장합니다.
*혈청 칼슘 수치(정상 상한치 초과): 1.0 mg/dL (0.25 mmol/L);
*DXA를 이용한 골밀도 측정: 요추, 고관절 전체, 대퇴경부 또는 요골 원위 1/3 부위의 T-점수 ≤2.5;
*X선, CT, MRI 또는 VFA 검사에서 확인된 척추 골절;
*크레아티닌 청소율 <60 cc/min;
*24시간 소변 칼슘 배설량 >400 mg/d (>10 mmol/d) 및 생화학적 결석 위험 분석에서 결석 위험 증가;
*X선, 초음파 또는 CT 검사에서 신결석 또는 신석회증이 확인된 경우;
50세 미만 이러한 합의 기반 미국 권고안의 근거를 고려하는 것이 중요합니다.
...
부갑상선 항진증을 동반한 부갑상선 선종

동대문구 답십리 우리안애, 우리안愛 내과, 건강검진 클리닉 내과 전문의 전병연
#동대문구내과 #성동구내과 #광진구내과 #답십리역 #장안평역 #용답역 #청량리역 #신답역 #한양대역 #왕십리역 #답십리사거리 #촬영소사거리 #전농동사거리 #내과 #국가검진 #위내시경 #대장내시경 #갑상선초음파 #복부초음파 #경동맥초음파 #심장초음파 #암검진 #래미안위브아파트 #엘림스퀘어 #두산아파트 #동아아파트 #한양아파트 #동답한신아파트 #두산위브아파트 #힐스테이트청계아파트 #래미안미드카운티 #청솔우성 #래미안크레시티 #롯데캐슬노블레스 #e편한세상답십리아르테포레
댓글