
목이 붓고 아프다?... 감기가 아니라, 튀어나와 있음!, 초음파로 확인; 턱밑 농양, 심경부감염 - 동대문구 답십리, 전농동, 우리안애 우리안愛 내과
- 10시간 전
- 7분 분량
70대 초반 남자
24년 2월부터 본원에서 혈압약등 투약중
감기진료도 자주 보는 편인데...
목아프고 부었다고 접수
그러나... 턱에서 튀어나온 모습이 보인다. 좌우 ~7 cm?
3일 되었고 아프다.
삼킬때 아프다.
누르면 압통, 튀어나온 아래쪽까지 압통은 연결해서 확인된다.


갑상선의 위치보다 위쪽으로 생각되나 같이해서 검사
갑상선내 비슷한 결절이 몇개 있는데 거의 등음영/약간 저음영의 결절인데 colloid particle과 microcalcification의 구별이 항상 어렵다고 생각된다. 19.1 mm로 크기도 어느정도 이상으므로, 추후 세침검사 고려라고 설명함

아니라고 생각했으나 악성세포가 나온 경우가 2례
좌측 턱밑샘에 결절/종양이 하나 있다. 아픈 원인과 같이해서 이비인후과 진료가 필요

턱의 중앙 위족에서 튀어나온곳에 아래와 같이 모습을 드려내는데

일부 낭성변화가 있으니 아래쪽으로 찌거기가 쌓여있는 것으로 봐도 될지...

그러나, 아래로만 있지는 않고 매달려 있는 모습니다.


제일 너비가 넓은 곳은 아래쪽에는 찌꺼기가 쌓인 곳도 있으며, 낭성변화가 크고 장성변화도 격벽이 있다.
주변으로 염증성 지방변화도 있어보인다.

모두 낭성변화는 아니므로 벽이 두꺼워 보이는 곳도 있다.

제일 아래쪽은 갑상선 연골 (thyroid cartilage) 높이인데 좌측으로 치우쳐 병변의 공간이 있다. 중앙에는 염증성 지방변화가 연결된다.

위아래 모습
공간의 주행방향, 아주 낭성의 부분과 내용물이 있는 곳의 혼재
lobulated contour

제일 아래쪽 주변의 염증성 지방변화, 압통은 병변 아래까지 연결된다. 염증성 변화가 얇게 더 내려가기 때문일것이다.

Neck ultrasound
양측 carotid artery 외측으로 특이한 소견 없음
왼쪽 submandibular gland내에 10.5 mm 크기의 mass가 관찰됨
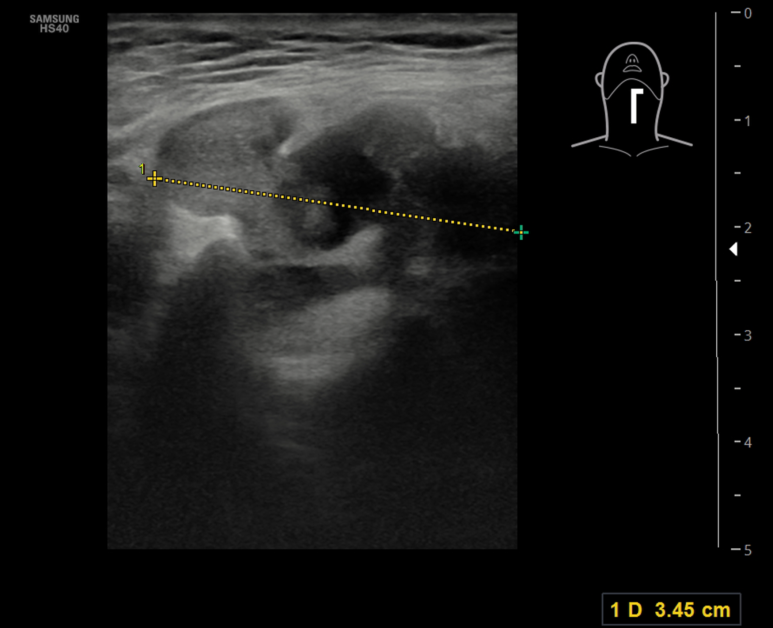
submandicular space에서 thyroid carilage까지 경계가 lobular하고 내부에 partially cystic한 종괴가 관찰됨 아래쪽 dependent area에 고음영의 debris로 생각되는 소견이 관찰됨, 위쪽에서는 붙어서 매달려 있는 고음영의 내용물, 일부 벽의 두께가 두껍게 관찰됨
thyroid cartilage 근방의 병변 주변에는 inflammatory fatty change가 관찰됨 (image25)
; 전체적으로 2.49*3.45 cm의 크기
1. 심경부감염 --> 응급실 방문, 평가 및 입원 치료, 필요시 수술의 결정
2. 침샘종양 --> 경부감염과 같이해서 이비인후과의 진료
3. 갑상선 결절 --> 본원에 다시 오면 세침 결정할수 있음
일부 낭성 변화가 있는 내부음영이 있는 불규칙한 경계를 가지며 주변에 염증성 지방변화라면 경부의 심부감염을 고려 응급실 방문하도록 안내하였다!
; 심경부 감염, 농양으로서는 처음 관찰하였다.
Despite a decrease in the incidence and mortality of deep neck infections (DNIs) as a result of the advent of antibiotics and improved dental care, these infections are not unusual and present a challenging problem because of the complex anatomy and potentially fatal complications that may occur.
항생제 도입과 치과 진료의 발전으로 심부경부 감염(DNI)의 발생률과 사망률이 감소했음에도 불구하고, 이러한 감염은 여전히 드물지 않게 발생합니다. 또한 복잡한 해부학적 구조와 치명적인 합병증을 유발할 수 있다는 점 때문에 치료에 있어 까다로운 문제를 안겨줍니다.
The deep neck spaces are regions of loose connective tissue filling the areas between the three layers of deep cervical fascia (superficial, middle, and deep layer). The fascial layers may limit the spread of infection. However, the spaces of the neck communicate with one another forming avenues by which infections may spread over large areas. An unsuspecting physician may underestimate an initially localized infection, which could shortly present as airway collapse or descending mediastinitis.
심경부 공간(deep neck spaces)은 심경부 근막의 세 층(표층, 중층, 심층) 사이를 채우고 있는 성긴 결합조직 영역입니다. 이러한 근막 층은 감염의 확산을 제한할 수 있습니다. 그러나 경부의 여러 공간은 서로 연결되어 있어 감염이 광범위한 영역으로 퍼질 수 있는 통로가 되기도 합니다.7 자칫 방심한 의료진은 초기에 국소적으로 나타난 감염을 과소평가할 수 있는데, 이는 곧 기도 폐쇄나 하행성 종격동염으로 급격히 진행될 위험이 있습니다.
Several reports have indicated that the origins of most DNIs are odontogenic infections. Consistent with this finding, the submandibular space is frequently involved in these infections. The submandibular space is limited above by the oral mucosa of the floor of the mouth and below by the superficial layer of the deep cervical fascia as it extends from the mandible to the hyoid bone. Mylohyoid muscle divides the submandibular space into the sublingual or superior space, containing the sublingual glands, the deep smaller portion of the submandibular gland, and Wharton’s duct, and the submaxillary or inferior space, containing the larger superficial portion of the submandibular space and its lymph nodes. These spaces communicate freely around the posterior border of the mylohyoid muscle. The submaxillary space may be further divided into a central submental space, between the anterior bellies of the digastric muscles, and lateral submaxillary spaces.
여러 보고에 따르면 대부분의 심경부 감염(DNI)은 치성 감염에서 기인합니다. 이러한 사실과 일치하게, 아랫턱밑공간, 악하공간, 악하 (submandibular space)은 이러한 감염에 흔히 관여하는 부위입니다. 악하극은 상부로는 구강저 점막과 경계를 이루며, 하부로는 하악골에서 설골로 이어지는 심경부 근막의 표층과 경계를 이룹니다. 악설골근(mylohyoid muscle)은 악하극을 설하극(또는 상부 공간)과 악하극(또는 하부 공간)으로 구분합니다. 설하극에는 설하선, 악하선의 심부 소엽 및 와튼관(Wharton’s duct)이 위치하며, 악하극(하부 공간)에는 악하선의 표층 대엽과 림프절이 위치합니다. 이 두 공간은 악설골근의 후방 경계를 통해 자유롭게 서로 연결됩니다. 악하극(하부 공간)은 다시 이복근(digastric muscle) 전복(anterior belly) 사이에 위치한 중앙의 이하극(submental space)과 측방의 악하극으로 세분될 수 있습니다.
As well as occurring secondary to dental infections, submandibular space infections may be a consequence of submandibular gland sialadenitis, lymphadenitis, trauma, or surgery. Furthermore, the submandibular space may be involved secondary to an infection that has developed in other deep neck spaces. Ludwig’s angina is a potentially life-threatening bilateral diffuse gangrenous cellulitis of the submandibular and sublingual spaces. It is named after the German physician, Wilhelm Frederick von Ludwig who first described this entity in 1836. In this condition, swelling of the submandibular tissues occurs rapidly and may cause an elevation of the tongue with consequent respiratory distress.
악하극(submandibular space) 감염은 치아 감염에 속발하여 발생할 뿐만 아니라, 악하선 타액선염, 림프절염, 외상 또는 수술의 결과로도 발생할 수 있습니다. 또한, 다른 심경부 공간(deep neck spaces)에서 발생한 감염이 파급되어 악하극을 침범할 수도 있습니다. 루드비히 협심증(Ludwig’s angina)은 악하극과 설하극(sublingual space)을 침범하는 양측성 미만성 괴저성 연조직염으로, 잠재적으로 생명을 위협할 수 있는 질환입니다. 이 질환은 1836년에 이를 처음 기술한 독일 의사 빌헬름 프레데릭 폰 루드비히(Wilhelm Frederick von Ludwig)의 이름을 따서 명명되었습니다. 이 상태에서는 악하 부위 조직의 부종이 급격히 진행되어 혀가 위로 밀려 올라갈 수 있으며, 그 결과 호흡 곤란이 초래될 수 있습니다.
The management of DNIs remains particularly troublesome due to the complex anatomy of the neck, polymicrobial etiology, and life-threatening complications that may arise. Furthermore, the inappropriate use of antibiotics, steroids, and nonsteroidal anti-inflammatory drugs may mask signs of infection and change the clinical presentation, making it more elusive, and also lead to a slow course of disease, delayed recovery, and the development of complications.
심경부 감염(DNI)은 복잡한 경부 해부학적 구조, 다균성 원인, 그리고 발생 가능한 치명적인 합병증으로 인해 치료 및 관리가 특히 까다롭습니다. 또한 항생제, 스테로이드, 비스테로이드성 항염증제(NSAID)를 부적절하게 사용할 경우 감염 징후가 은폐되거나 임상 양상이 변화하여 진단을 어렵게 만들 수 있으며, 질병 경과를 지연시키고 회복을 늦추거나 합병증을 유발할 수도 있습니다.
The mainstay of treatment of DNIs consists of airway control, antibiotic medical treatment, and, if necessary, surgical drainage. The maintenance of a safe and secure airway is mandatory in submandibular space infections. In patients with bilateral submandibular swelling, an airway obstruction can be the result of the tongue pushing against the roof of the mouth and the posterior pharyngeal wall, or be a consequence of anterior visceral space involvement with laryngeal edema.
심경부 감염(DNI) 치료의 주축은 기도 확보, 항생제 투여, 그리고 필요한 경우 시행하는 수술적 배농입니다. 특히 악하 공간 감염 시에는 안전하고 확실한 기도를 유지하는 것이 필수적입니다. 양측성 악하 부종이 있는 환자의 경우, 혀가 구개 및 후인두벽 쪽으로 밀려나거나 전내장 공간(anterior visceral space)으로 감염이 확산되어 후두 부종이 동반됨으로써 기도 폐쇄가 발생할 수 있습니다.
Open surgical incision and drainage are considered the mainstay of treatment for submandibular space abscesses and Ludwig’s angina. Currently, our philosophy is to treat all patients with large doses of broad-spectrum intravenous antibiotics (e.g., amoxicillin/clavulanate potassium) until culture results identify the causative organism. In cases of large abscesses or multiple space involvement, an open surgical incision and drainage are promptly performed. In patients with small abscesses, a watch and wait policy is applied for 48 hours; if a lack of response to medical treatment is noted both clinically and by CECT, the patient is treated with an open surgical drainage.
악하 공간 농양(submandibular space abscess)과 루드비히 협심증(Ludwig’s angina) 치료의 주된 방법은 개방적 절개 및 배농술입니다. 현재 본원의 치료 방침은 원인균이 배양 검사를 통해 확인될 때까지 모든 환자에게 광범위 항생제(예: 아목시실린/클라불란산 칼륨)를 고용량으로 투여하는 것입니다. 농양의 크기가 크거나 여러 공간을 침범한 경우에는 즉시 개방적 절개 및 배농술을 시행합니다. 농양의 크기가 작은 환자의 경우 48시간 동안 경과를 관찰하며, 임상적 소견 및 조영 증강 CT(CECT) 검사상 약물 치료에 대한 반응이 없는 것으로 확인되면 개방적 배농술을 시행합니다.
In conclusion, submandibular space infections are potentially lethal infections. Physicians should be aware that the clinical status may quickly and unexpectedly worsen. Airway obstruction and spread of infection to the mediastinum are the most troublesome complications. Therefore, the maintenance of a secure airway is paramount and an aggressive treatment is justified. Patients with cellulitis and small abscesses can respond to antibiotics alone. A surgical drainage should be performed in patients with larger abscesses, Ludwig’s angina, anterior visceral space involvement, and in those who do not respond to antibiotic treatment. Nonetheless, each case has to be taken on its merit. Specifically, the clinical assessment in patients with comorbidities, especially diabetes mellitus, requires a high level of suspicion for potential life-threatening complications. In these patients an early surgical drainage should always be considered, even in seemingly less critical cases.
결론적으로, 악하 공간(submandibular space) 감염은 잠재적으로 치명적인 질환입니다. 의료진은 환자의 임상 상태가 예기치 않게 급격히 악화될 수 있음을 인지해야 합니다. 기도 폐쇄와 종격동으로의 감염 확산은 가장 우려되는 합병증입니다. 따라서 안정적인 기도를 확보하는 것이 무엇보다 중요하며, 적극적인 치료가 필요합니다. 봉와직염이나 작은 농양을 동반한 환자는 항생제 치료만으로도 호전될 수 있습니다. 그러나 더 큰 농양, 루드비히 협심증(Ludwig’s angina), 전방 내장 공간(anterior visceral space)으로의 감염 확산이 있거나 항생제 치료에 반응하지 않는 경우에는 수술적 배농을 시행해야 합니다. 그럼에도 불구하고 각 사례는 개별적인 상황에 맞춰 판단해야 합니다. 특히 당뇨병과 같은 기저 질환이 있는 환자의 경우, 생명을 위협할 수 있는 합병증의 가능성을 염두에 두고 면밀히 임상적 평가를 수행해야 합니다. 이러한 환자들에게는 비록 증상이 경미해 보이더라도 항상 조기 수술적 배농을 고려해야 합니다.

...
농양은 없이 심부경부감염, 좌측 턱밑샘 구획, submandibular space
동대문구 답십리 우리안애, 우리안愛 내과, 건강검진 클리닉 내과 전문의 전병연
#동대문구내과 #성동구내과 #광진구내과 #답십리역 #장안평역 #용답역 #청량리역 #신답역 #한양대역 #왕십리역 #답십리사거리 #촬영소사거리 #전농동사거리 #내과 #국가검진 #위내시경 #대장내시경 #갑상선초음파 #복부초음파 #경동맥초음파 #심장초음파 #암검진 #래미안위브아파트 #엘림스퀘어 #두산아파트 #동아아파트 #한양아파트 #동답한신아파트 #두산위브아파트 #힐스테이트청계아파트 #래미안미드카운티 #청솔우성 #래미안크레시티 #롯데캐슬노블레스 #e편한세상답십리아르테포레
댓글